The evidence behind gadolinium MRI contrast, and why “it helped millions” is a claim no study can support.
The short version
This week, the Daily Mail's Health Supplement ran a feature on patients who say they have been harmed by gadolinium, the contrast agent injected in up to half of all MRI scans. I was one of the patients interviewed, alongside Professor Brent Wagner, a nephrologist who studies gadolinium toxicity, and Dr Giles Roditi, a consultant radiologist who defended the agents.
Dr Roditi made a claim that deserves a closer look: that "millions who have had GBCAs have been helped and diagnosed as a result." It is the sort of sentence that sounds unanswerable. It is also a number that, as far as the published evidence goes, nobody can find. What the literature actually measures is the opposite: how often the contrast adds nothing at all.
This post is about that gap. It is educational, it is not medical advice, and it is grounded in peer-reviewed studies you can read for yourself.
Even Professor Wagner, who is clear that he does not want these agents banned, draws one firm line:
"people have the right to know what they are being injected with."
Why this matters to you

If you have had an MRI with contrast and felt unwell afterwards, you have probably been told one of two things. Either that gadolinium leaves the body within hours, or that your symptoms cannot be the dye because the dye is safe and necessary. You may have been told both in the same appointment, by the same person, without anyone noticing the contradiction.
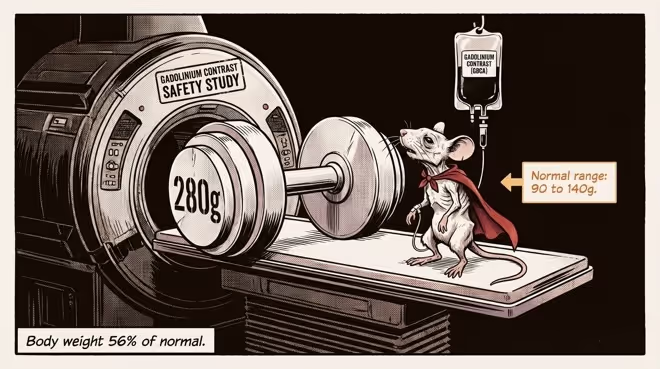
I have been on the receiving end of that conversation. After an MRI in Belfast in November 2016, I went from lifting weights to having no muscle strength, from sleeping soundly to lying awake with a body that felt, in the words I used in the Daily Mail, electrified. My labs were normal. My experience was not.
What helped me most was not reassurance. It was evidence. So let me give you some.
What gadolinium is, briefly
Gadolinium is a toxic heavy metal. To make it safe enough to inject, it is wrapped in a binding molecule, a process called chelation, so that it can be passed out in urine before it does harm. The theory is that the wrapping holds and the metal leaves. For most people, most of the time, much of it does.
The trouble lives in the words "most" and "much." A growing body of research shows that gadolinium is retained in the brain, bone, skin and other organs, including in people with perfectly normal kidneys. That is the foundation of what is now called gadolinium deposition disease. Retention is real, and it matters. But whether the retained metal is the cause of lasting illness, or the spark that lit a larger fire, is a question I will come back to, because the answer changes how you get well.
The number nobody can find

Here is the claim again: millions helped and diagnosed. Now, here is what happens when you go looking for the studies behind it.
You do not find a study that counts the millions. You find study after study counting the scans where the contrast made no difference.
In paediatric pituitary MRI, about 85% of lesions were visible without any contrast at all. Gadolinium revealed a lesion that was not otherwise visible in 0.18% of patients, a single microadenoma in the whole cohort. The authors concluded that in most cases the contrast was simply unnecessary (Mallmann et al., 2021).
In prostate MRI, when radiologists checked the non-contrast MRI images on the computer screen before deciding whether or not to go ahead with contrast, 75.8% of patients did not need gadolinium at all. Sensitivity barely moved: 98.3% with the streamlined approach against 99.2% with routine contrast, no significant difference, with no loss in cancer detection (Engels et al., 2025).
For prostate cancer diagnosis more broadly, a systematic review and meta-analysis found that bi-parametric MRI without gadolinium matches contrast-enhanced multiparametric MRI for clinically significant cancer, the kind that actually matters, with only a small drop in overall sensitivity (0.77 versus 0.84) that the authors judged an acceptable trade-off for avoiding contrast. This is why contrast-free protocols are increasingly standard (Liang et al., Transl Androl Urol 2020).
For osteomyelitis in the limbs, a systematic review found no evidence that gadolinium added diagnostic value at all (Systematic review, 2021).
Notice that even these studies are arguing on the contrast's home turf. They are measuring detection: did gadolinium help the radiologist see something? And the answer, in these settings, is often no. But there is a deeper problem beneath the surface, and it is the one that matters most.
Detection was never the point
When gadolinium's defenders reach for its strongholds, they name breast MRI, active multiple sclerosis lesions, cancer staging, vascular imaging. In each, the claim is that contrast lets you see more. Park that for a moment. Seeing more is not the same as living longer or suffering less. Detection is a surrogate. The question that actually matters is whether finding the thing changed what happened to the patient... for the better... AND that the patient's outcomes then improve as a result. On that question, the evidence is thin to absent.
In breast screening, the US Preventive Services Task Force found no studies of supplemental MRI reporting on mortality or morbidity at all (USPSTF). The case for it rests entirely on detection, and it is worth being clear about what is being detected. Much of what breast MRI finds is ductal carcinoma in situ, or DCIS: abnormal cells sitting inside a milk duct that have not broken through its wall. It is filed under "cancer," and the word lands like a verdict, but DCIS is not invasive cancer. It cannot be felt as a lump, it causes no symptoms, and a large share of it would never spread, never progress, and never shorten the life of the woman carrying it. So ask the plain question: what does she gain by being told it is there? On the page, very little. What she stands to lose is concrete. She is told she has cancer, which is frightening enough on its own that many people are put on antidepressants to cope, and antidepressants are not sweets, however freely they are handed out. From there, most women are sent down a pathway of surgery and radiotherapy, each carrying its own real risks. And choosing to avoid surgery and simply watch the lesion is no escape from intervention: active surveillance commits a woman to years of serial breast MRI, dependent on gadolinium contrast, to monitor a lesion that in most cases was never going to progress (active surveillance of DCIS, 2024). Estimates of how much screen-detected DCIS is overdiagnosis run from 20% to 91%, and because DCIS is almost always treated, every overdiagnosis becomes an overtreatment: surgery, radiation, sometimes a contrast reaction, always the fear (overdiagnosis modelling, 2025). In a screening setting, better detection can cost more health than it saves.
In multiple sclerosis, gadolinium enhancement lights up active plaques, and it is natural to assume that seeing them must somehow help you stay well. Here is the hard part. If you are hoping that a contrast scan will help keep you out of a wheelchair, hold on to your mobility and your independence, or protect your quality of life, the evidence does not support that hope. A Lancet meta-analysis found that enhancing lesions, while a moderate predictor of short-term relapses, are a poor predictor of the cumulative disability and impairment that actually shape a life (Kappos et al., Gadolinium MRI Meta-analysis Group, Lancet 1999). Seeing the plaque is not the same as changing what it does to you.
In vascular imaging, the job is to map the blood vessels and the lesions within them, and gadolinium is widely assumed to be the only way to do it sharply. It is not. Non-contrast sequences such as quiescent-interval single-shot angiography map the vessels just as well: in peripheral artery disease, the accuracy of non-contrast QISS was not statistically different from catheter angiography, the gold standard, and comparable to CT angiography (sensitivity 84% against 89%). Nothing is missed for want of gadolinium (QISS angiography study, 2016). This is not abstract. David Mallon, the father of four whose story opened the Daily Mail feature, had life-saving surgery for a tangle of brain blood vessels and was then given scan after scan to monitor them, dating the collapse of his health to the hours after the first. The setting in which he was exposed again and again is precisely the one where the contrast had the least to add.
In cancer staging, a contrast-friendly Stanford group asked outright whether gadolinium is necessary to stage childhood tumours. Across 119 children, unenhanced imaging matched the contrast-enhanced scans on every diagnostic criterion: liver metastases 84.6% versus 85.7%, lymph nodes 84.9% either way, bone marrow 94.1% versus 91%. Where the children also had a PET scan, the PET and the gadolinium agreed 86% of the time, so the contrast added little that the PET had not already shown. The authors concluded that gadolinium "is not necessary for accurate diagnostic characterisation of most solid pediatric malignancies," with focal liver lesions the only stated exception. Survival and morbidity were never assessed (Klenk et al., J Nucl Med 2016).
Behind every one of those percentages is a person. David Mallon is one of them.
"It's ruining my life. I still have joint pain, brain fog, memory loss and problems with my vision."
So the honest summary is not "gadolinium never helps." It is something more precise and more damning. The benefit repeatedly claimed for it is a benefit of detection, and detection has been allowed to stand in for outcomes without ever being asked to prove it improves them: whether anyone lives longer, suffers less, stays out of a wheelchair, keeps their independence, or holds on to the life they had. The burden of proof belongs to the people who made the injection routine. On the measure that matters, lives and morbidity, that proof has not been met.
There is a further turn of the screw, and it is worth understanding, because it's where the comfort hides. When a benefit for finding disease earlier is claimed, it usually rests on counting deaths from the one disease being scanned for. That number is easier to massage than it looks. If the treatment that follows the scan causes a fatal heart attack or a fatal infection, the death is often recorded against the heart or the infection, not the cancer, and it quietly leaves the scoreboard. If someone is diagnosed with a lesion that would never have harmed them, then dies of despair or a heart attack in the shock of the diagnosis, the figures still count them among the lives the screening saved. The only measure immune to this is all-cause mortality, every death from any cause, and on that measure, routine contrast has, as far as I can find, never been tested at all. Nor is the diagnosis itself the neutral event it's treated as: in the week after a cancer diagnosis, suicide runs around twelve times higher and fatal heart attacks more than five times higher than normal (Fang et al., New England Journal of Medicine, 2012).
And so the asymmetry sharpens. The people who say it has helped millions cannot produce the number. The people who actually measured its value keep finding either that it changed nothing the radiologist could see, or that what it let them see changed nothing for the patient. One side has a round figure and a reassuring tone. The other side has percentages, sample sizes and journals.
The evidence that runs the other way
Set the cancer question aside for a moment and ask what people actually hope an MRI will protect. Not an image. Their sleep. Their energy. Their mood. The ability to keep working, to progress in a career, to keep their place in their own life. And alongside that, the symptoms they hope to be spared: neurological, inflammatory, connective-tissue and hormonal.
No study shows that contrast improves a single one of them. The observational evidence points the other way. In the largest patient-led survey of its kind, 324 participants, which I co-authored, people who had gadolinium contrast reported exactly the burdens an MRI is meant to spare them: tingling and prickling, brain fog and cognitive problems, burning pain, crushing fatigue, joint pain, each reported by between roughly half and four-fifths of respondents. The toll fell on lives, not only on symptoms: 43% had a change in employment status, 41% said altered memory and brain function had changed their ability to work as they once did, and new diagnoses arrived after the scan, hormonal, inflammatory and neurological alike, from Hashimoto's and hypothyroidism to mast cell activation and small-fibre neuropathy. And 24% had considered suicide (patient survey report).
It is worth naming who gets counted as proof. Patients are routinely told their symptoms cannot be the gadolinium unless they can produce a test showing the metal was retained, as though illness only counts once you can exhibit the residue. No other corner of medicine works this way. We do not ask a person harmed by a drug to first present the molecule in their tissue, and the profession that demands it here is the same one that took twenty years to notice nephrogenic systemic fibrosis at all. So when the survey is split by who had a positive retention test, the pattern is revealing: that group was not a purer sample of the harmed but the sickest, the most likely to have been dismissed as psychosomatic, and the most likely to have considered suicide. That is not coincidence. Someone who is disbelieved goes looking for proof they are not imagining it, and a test result is often the only thing that buys them a hearing, before, too often, the next doctor waves even that away and reaches for the antidepressant pad. The retention did not make them ill. Being disbelieved sent them hunting for it. And the symptoms were there regardless: even among those who never obtained such a test, 62% reported the tingling, 59% the brain fog, 53% the fatigue.
A patient-led survey cannot prove cause, and I will not pretend it does. It is self-reported, and the people drawn to fill it in are people who already suspect they were harmed. But that is exactly why the direction is worth noticing. If contrast were the benign and largely irrelevant additive its defenders describe, the harms these patients live with would scatter in every direction and form no pattern. Instead, the pattern is consistent, pointing one way, and it's the precise opposite of what anyone lying in the scanner is hoping for. The honest position is not "contrast harms these things, proven." It's that contrasts have never been shown to help them, and the only structured evidence we have suggests they may do the reverse. Not a comfortable place for a routine injection to sit.
But isn't it cancer or the contrast?
Read the comments under any piece like this one, and the same argument rises again and again, almost word for word: would you rather risk a little contrast, which is very safe, or miss a cancer and die? It is offered as the end of the conversation. It deserves to be slowed down, because it is built from several moves, and not one of them holds.
It conflates the scan with the dye. An MRI and the gadolinium injected during some of them are not the same thing. Around half of MRI scans use no contrast at all, and among those that do, study after study finds large fractions did not need it. The machine that finds the tumour works without the dye far more often than the public has ever been told. "MRIs save lives" is true and beside the point. The question on the table is the gadolinium, not the magnet.
It offers two doors when there are three. The choice is staged as contrast or catastrophe. The option the evidence actually supports, the same scan without contrast, or with contrast only where it changes what the doctor does next, is quietly removed from the room. As the studies above show, for large fractions of scans, that third door opens onto exactly the same diagnosis.
It leans on "I have had fifty, and I am fine." Accounts of people who feel well after many scans land like proof, and they are not. A harm that strikes a minority is entirely compatible with most people being fine. The well are exactly what you would see whether the true rate is zero or one in twenty. And almost nobody who feels fine is quietly auditing their sleep, energy and mood against the life they would otherwise have had. That gap is the very reason a structured survey exists, and the survey did not find reassurance.
It treats "it might be your illness, not the dye" as an answer. This is the move Dr Roditi himself reached for in the feature:
"Someone has an MRI because they have arthritis, then afterwards they experience joint pain which they are convinced is caused by the GBCA, not the condition they suffer from."
Sometimes symptoms do come from the disease that prompted the scan. But this line is only ever reached for, never tested. It cannot explain why the same cluster of complaints recurs across thousands of unconnected patients, and it could be settled tomorrow by the contrast-versus-no-contrast randomised, placebo-controlled, clinical trial that nobody has run. Until then, it is an assertion, not a finding, and it happens to be the assertion that asks no one to change anything.
It assumes the benefit it is meant to prove. "Doctors weigh risk against benefit, lowest dose, kidney function checked" describes real and careful practice, but it takes for granted that the benefit side of the scale is filled in. For outcomes, it is blank. You cannot weigh an unknown risk, small or otherwise, against a benefit no one has ever measured and announce that the answer is obviously favourable.
None of this means refuse every scan, or distrust everyone in a white coat. It means the cancer-or-contrast question is the wrong question, carrying its own answer smuggled inside it. The right question is narrower, and it can actually be answered: for this scan, for this person, does the gadolinium change what happens next? Often it does not. Not to mention the big question anyone facing a potential cancer diagnosis wants resolved, but which the current research cannot answer: Will the contrast save my life? You are allowed to ask.
How an unsourced number survives
You might reasonably ask how a claim like that gets printed at all. The answer is mundane. It was an interview quote, not a published statement. Newspapers print attributed opinion under far looser rules than a journal. There is no peer review of a quote, no requirement to cite a source, and "millions have been helped" is vague enough to be unfalsifiable. Nobody fact-checks a round number that flatters the status quo.
This is not a conspiracy. It is something quieter and more durable: a profession's sincere belief, repeated until it feels like data. Most clinicians who defend gadolinium are not being dishonest. They are protecting a tool they trust, and trusting a tool you use every day is far more comfortable than entertaining the thought that it has been quietly harming some of the people you treated. Denial is the cheapest defence against that particular grief. It is also paid for by the patient.
The oxalate connection, and a fact worth knowing
The most interesting science in the Daily Mail piece came from Professor Wagner, whose work suggests a mechanism for how the metal escapes its wrapping. The culprit he points to is oxalate, an organic acid found in many plant foods, which appears to help separate gadolinium from its chelate, allowing the free metal to bind with calcium and form tiny crystals that lodge in tissue.
This matters to me because oxalate has been central to my own recovery and to the work I now do. And there is a detail here that almost nobody is told. Excess vitamin C is converted in the body into oxalate. Ascorbic acid is metabolised to oxalic acid, and controlled studies show that higher intakes measurably raise the oxalate your body has to deal with, with ascorbic acid estimated to account for around 40% of the oxalate the body makes for itself (review of oxalate precursors, 2021). So the well-meaning person who loads up on vitamin C may be quietly raising the very acid implicated in setting gadolinium free.
I would not reduce this to a single rule about juice on the morning of a scan. The deeper point is about oxalate load over years, the "healthy" plant-heavy diets that carry far more of it than anyone realises, and the vulnerability that may build long before the MRI ever happens. That is a longer story, and it is the one I spend most of my time on now.
The spark, not the fire
Here, I have to part company with the way this is usually told, gently including the way my own story reads in the newspaper. The standard picture treats retained gadolinium as the illness itself: metal lodges in tissue, metal makes you sick, remove the metal, and you recover. After years in this, my own and many others', I no longer think that is quite right, and the difference is not academic. It changes how you try to get well.
In the way I have come to understand it, the contrast agent is the trigger, not the engine. The spark, the kindling, the seed crystal dropped into a body that was already saturated and vulnerable, often from years of oxalate and the slow accumulation of modern life. What the spark sets off is a self-feeding cascade: crystallisation in the tissues, an immune system that turns on its own, emergency responses built to last hours that instead run for years. Once that fire is lit, it sustains itself. It becomes an ouroboros, the serpent swallowing its own tail. At which point, the gadolinium still sitting in your bones is less the engine of the illness than the ash that proves there was a fire. It is a marker that the cascade was triggered and is still burning, not, by itself, the thing keeping you ill. Or at the very least, not on its own.
This is why chasing the metal alone so often disappoints, and why recovery, mine and my clients', has come instead from calming the whole cascade: the diet, the oxalate, the nervous system, the accumulated load. I call this framework ATTRACT, and it is far too large a story for the end of one blog post. But it is the reason I no longer ask only, "How do I get the gadolinium out," and ask instead, "How do I put the fire out?"
What I want you to take from this

Your body is not your enemy, and it is not making it up. Real damage can occur, from retained metal, from oxalate, from the long grind of modern life on an ancient biology. But many of the symptoms that torment people after a scan are not the damage itself. They are the body's emergency responses, salvage operations meant to keep you alive, running far longer than they were ever designed to. Understanding that is the first step to relieving the siege rather than fighting yourself.
And when someone in a white coat tells you a comfortable round number, you are allowed to ask the most powerful question in medicine. Where is the evidence? Sometimes there is a good answer. Sometimes, as here, the silence tells you everything.
"Gadolinium doesn't just take your health, it takes your life as you knew it."
About the author
Dr Catriona Walsh is a Cambridge-trained physician and former NHS consultant paediatrician who now works as a nutrition and lifestyle coach at The Food Phoenix. She co-authored the largest patient-led survey of symptoms following gadolinium contrast MRI (324 patients), collaborates with Professor Brent Wagner's team on gadolinium pathophysiology and Dr Susan Owens on oxalate toxicity, and is the author of Contrasts: More Than Meets the MRI. She has been featured on Sky News, BBC Radio Ulster and in the Daily Mail. ORCID: 0009-0005-0215-207X.
If this is your story
If you suspect gadolinium or oxalate is part of what happened to you, you do not have to work it out alone at two in the morning. Start with a free, no-pressure Comprehensive Health Assessment. You can also read the MRI Contrast Guide, download the patient survey report, or read my book, Contrasts: More Than Meets the MRI.
Frequently asked questions
Does gadolinium leave the body after an MRI?
Much of it does, particularly in people with healthy kidneys, but research now shows gadolinium is retained in the brain, bone and other tissues even when kidney function is normal. The old reassurance that all of it is gone within hours does not match the evidence.
Is MRI contrast always necessary?
No. For many indications, including much prostate and paediatric pituitary imaging, peer-reviewed studies show gadolinium can be omitted in the large majority of cases without losing diagnostic accuracy. Even in the settings where it is most defended, such as breast, multiple sclerosis and vascular imaging, the benefit that has been demonstrated is occasional better detection, not better patient outcomes. Whether finding more changes how long or how well a patient lives is a separate question that those studies largely did not ask.
Does gadolinium contrast save lives?
No one has shown that it does. There is no trial comparing scans with contrast against scans without it that measured whether patients lived longer or suffered less. The benefits that are claimed are infrequent benefits of detection, seeing more clearly, which is not the same thing. Until that trial exists, the life-saving benefit of routine contrast is assumed, not proven.
What is gadolinium deposition disease?
A pattern of symptoms reported by some patients after gadolinium contrast, including fatigue, brain fog, joint and muscle pain, and cognitive difficulties, associated with retained gadolinium in people with normal kidney function. It is conventionally treated as a thing apart from nephrogenic systemic fibrosis, the condition recognised in kidney failure, but I do not see a clean line between them. In the survey I co-authored, 19 of the 28 most frequent NSF symptoms were also top-ranked by patients with normal kidneys, which is why we argue this is not two separate diseases but one gadolinium-induced illness of varying severity, a "disease of degrees." In my own model, the retained gadolinium is best understood as the trigger, and a lasting marker, of a wider self-sustaining cascade, rather than the engine that keeps the illness running. I explain that in my short ATTRACT explainer
Can diet affect gadolinium toxicity?
Emerging research links oxalate, an acid found in many plant foods, to the release of gadolinium from its protective chelate. Excess vitamin C is also converted into oxalate in the body. This is an active area of research rather than settled fact, and it should be approached carefully, because reducing oxalate too quickly can cause its own problems.
Isn't an MRI with contrast safer than missing a cancer?
This is the wrong question, and it hides its own answer inside it. It treats the scan and the dye as the same thing, when they are not. Around half of MRI scans use no contrast at all, and among those that do, study after study finds large fractions did not need it. So the real choice is rarely contrast or a missed cancer. It is usually the same scan with or without gadolinium, reaching the same diagnosis. Contrast may have its place, but it should be the answer to specific questions, not a routine you are talked into: